This is a miniseries about why the statistics on this site, and the upcoming website, should matter to you, not only in your everyday life, but in preventing child sexual abuse... before it can happen.
Statistic 1: Most Abusers Are Those Known And Trusted
To be specific, 90-93% of child sexual abuse is committed by those known and trusted by the victim. This one is probably the single most important statistic to the prevention of child sexual abuse: The common myth is that it is strangers you need to worry about, and teaching stranger danger is rampant. Well, I grew up in that era of stranger danger. It did not protect me from the three times I was sexually abused by those I knew and trusted.
This single statistic means also that mandatory reporting laws will always impede the prevention of abuse, because it means that those who may be in need of mental health help do not get that help. Why? Because most abusers are those known and trusted, you will not report your son to the police for fondling a younger sibling. You will not want to ruin the rest of his life. The same holds true for the husband, the uncle, the teacher, the babysitter, etc.
Statistic 2: Prevalence Of Sexual Abuse
The prevalence of child sexual abuse has been reported in a number of ways. Studies indicate that the victim-reported abuse on surveys is around 8% for boys, and 19% for girls. Estimates that attempt to account for underreporting put abuse at one in six boys, and one in four girls. This statistic is important for obvious reasons. It teaches us that underreporting is real, and that the true prevalence of child sexual abuse in any society will likely never be known. It teaches us that boys are victims of sexual abuse, and that they report less due to a myriad of complex sociological factors.
But let us practically apply that statistic, just to the United States:
According to this source, there are 73.8 million children in the United States, and the known victim-reported prevalence (8%, 19%) translates to roughly 3,011,040 boys and 6,870,780 girls, or 9,881,820 children. The
estimate that attempts to account for underreporting (38-50% ARE
reported, so we will assume for the moment that only 38% are reported)
translates to 16,008,548
children.
In other words, our best data and estimates indicate that 13.39-21.69% of children are sexually abused (which is a big deal).
In other words, our best data and estimates indicate that 13.39-21.69% of children are sexually abused (which is a big deal).In other words, our best data and estimates indicate that 13.39-21.69% of children are sexually abused (which is a big deal).
In other words, our best data and estimates indicate that 13.39-21.69% of children are sexually abused (which is a big deal).
In other words, our best data and estimates indicate that 13.39-21.69% of children are sexually abused (which is a big deal).
Most of all, the prevalence of child sexual abuse shows us that too many children are affected by this epidemic already for us to be reacting to abuse after it happens. After abuse happens is clearly not good enough.
Statistic 3: Most Abuse Happens In A Residence, One-On-One
The circumstances of abuse can be shocking to some: 77% of child sexual abuse is done in a residence, and 81% of child sexual abuse occurs in a one-on-one situation. This is vitally important for prevention and for policymakers, because it means that the majority of abuse does not happen in parks, schools, playgrounds, libraries, movie theaters, or businesses. Restricting people from any of these places does nothing to stop sexual abuse, because not only does abuse not happen in these places, abuse is more often perpetrated not by strangers, but by someone the child knows.
Statistic 4: False Allegations Are Extremely Rare
How rare, you ask? Think 4-8%, and typically those false reports are allegations originating with an adult in the child's live, not the child themselves. What this clearly demonstrates is that children can be trusted to tell the truth about being sexually abused. If a child has told you they were abused, you must treat it as a fact and respond accordingly by going to a therapist with expertise in sexual abuse victims, a child advocacy center, Child Protective Services, or the police. While no doubt, given statistic number one, you know and trust the abuser, the fact of the matter is that they need treatment and help, and they will not get that without the police being at least notified. This statistic is obvious: Believe a child's allegation of sexual abuse.
Wrapping Up
While there are many more statistics in child sexual abuse that matter a great deal, these four statistics and why they matter form the core of what the average person absolutely must know about child sexual abuse. By being aware of not just the fact and figure, but why that figure is important, you can become involved in preventing child sexual abuse... before it can happen.
All the time, you hear statistics about a great number of things. You see them frequently here, on the blog. But you do not often see the practical application of them, and it is up to you to figure out the point of the statistic in question. Some are obvious, while others are not nearly as obvious.
Because of that, I will do a miniseries on why the statistics cited on this site should matter to you, not only in your everyday life, but why they matter to preventing child sexual abuse.
Statistic 1: Population Of Pedophiles
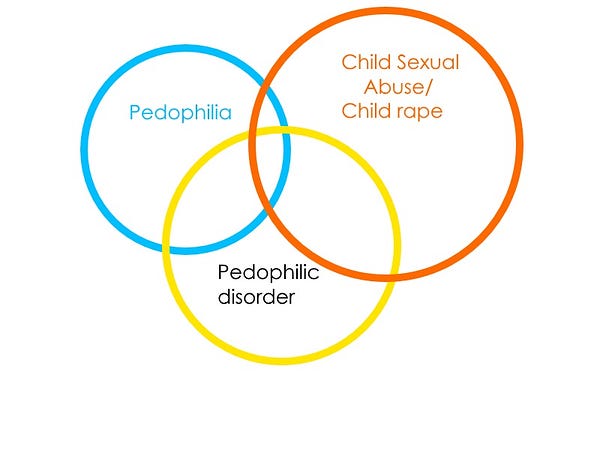
Current statistics (the DSM-V (the psychiatry Bible) and Michael Seto) put the population of those with pedophilic disorder as mainly being male: 3-5% of adolescent and adult males. This is, of course, an estimate. However, it is telling because pedophilic disorder is not the same thing as pedophilia: The DSM-V differentiates the two. This means that the high estimate of 3-5% of males means that even more have a sexual attraction to children. Why? Because pedophilic disorder is a very specific mental condition in which those with pedophilia, a sexual attraction to prepubescent children, have difficulties like depression, anxiety, and difficulty relating to others. It does not cover those with an attraction to teenagers, which means that the true population figure for those with attractions to children broadly is actually higher than 3-5% of males. That is about to matter even more because of statistic number two...
Statistic 2: Proportion Of Those Who Sexually Abused Children Who Have Pedophilia
The second statistic is well-known by researchers and therapists working with forensic and non-forensic populations of pedophiles: One-third of those who sexually abused children have pedophilia. Yes, one-third. This tells us a great deal of information about child sexual abuse: Mainly, that it is not about getting sexual pleasure from a child. You see, if the population of those with pedophilic disorder is an estimate and a low one, but the proportion of abusers with pedophilia is proportionately higher than that estimate (6-15 times higher). This means there is something associated with the attraction that drives the motivating factors that fuel the decision to abuse a child.
Statistic 3: Most Who Have Pedophilic Disorder Do Not Abuse Children
If you were to read through the section on pedophilic disorder in the DSM-V, you see a rather bleak picture of a person tortured by their attractions to children. When you get to the differential diagnosis section, you see that pedophilic disorder can correlate to alcohol and substance abuse, obsessive-compulsive disorder, and even antisocial personality disorder. When you get to comorbidity, you see that pedophilic disorder is correlated to depression, bipolar, and anxiety disorders... while they also note that these observations are only among forensic populations of those with pedophilic disorder, meaning that more study is needed in this area.
You have heard me state on this blog before: Given our best estimates without trying to compensate for underreporting, 3-5.2% of pedophiles molest children, and after accounting for that, 4.8-9.36% molest children. In other words, our best guess is that 90.64-97% of pedophiles do not molest children. This is obviously significant, because it means that a sexual attraction to children does not appear to frequently correlate with sexual abuse. It also means that what I just outlined from the DSM-V about the bleak lives of someone with a sexual attraction to children... only comes from looking at 3-10% of those with such an attraction. In other words, a lot of our information is missing about pedophilia, sexual attraction to children in general, and most importantly, it is not reasonable to correlate pedophiles with child molestation. It means that a sexual attraction to children is more common than child sexual abuse. This is frankly huge, not only for those who study pedophiles and pedophilia, but also for child sexual abuse prevention.
Statistic 4: Those Viewing Sexual Abuse Images More Often Have Pedophilia...
To be precise, 61% of those convicted of possessing child sexual exploitation material have pedophilia. What this means is that pedophiles are trying to satisfy their sexual needs with sexual material of children. This begs the question, given recent discussion around art, virtual reality, and 3-D images involving children, of whether researchers are wrong to assume that such virtual imagery serves as a gateway for a hands-on offense involving a child. If more pedophiles view sexual imagery involving real children, could that number be reduced if virtual imagery involving children were more available, and legal? Could this virtual imagery be not only a better outlet than imagery involving real children, but reduce the number of sexual abuse cases? More study is clearly needed in this area to test correlation.
Enough Statistics: What Is The Point?
The point to overviewing just these three statistics and why they matter is not merely an academic exercise: It has real implications for preventing child sexual abuse. It suggests that stigmatizing a sexual attraction to children and viewing it as a risk factor for sexually harming children is not going to be helpful to preventing child sexual abuse, because a sexual attraction to children is less often a risk factor for a hands-on sexual abuse case and more often a risk factor for viewing sexual abuse images. While viewing images of children being sexually abused is indeed harmful to the children involved, the creation of virtual images is not because real children are not involved.
These statistics also very clearly indicate that we have barely scratched the surface of knowing pedophilia and sexual attraction to children: It means more study is sorely needed in a variety of ways to uncover that knowledge. It means we should look at what happens when you give those with a sexual attraction to children support instead of an automatic and clearly incorrect label of child molester, as Prevention Project Dunkelfeld is doing in Germany. It is obvious to anyone working in these areas... they need money to do this research, and the number of people willing to put money towards this research is limited.
Bottom Line
Conflating a sexual attraction to children, which we barely know much about, with the sexual abuse of a child spreads incorrect myths that hamper our ability to prevent sexual abuse and interfere with the ability of those with an attraction to children to seek support and seek peers who face the same attraction. Mixing up the sexual attraction to children, with the sexual abuse of a child, is unwarranted, inaccurate, and only serves to enable child sexual abuse by driving both issues further into darkness and secrecy, where sexual abuse thrives.
What You Do Not Know About Pedophiles Could Spare Children Sexual Abuse
Many, many times our knowledge of something is incomplete. When that happens, we avoid taking an action when we would do so with that knowledge we are missing. We can also take action when we would not do so with that knowledge we lack. Worse, we can take action based entirely on how we feel, which can lead to disastrous consequences.
You could spare a child the pain of abuse with your knowledge.
So how does that play out in the case of child sexual abuse, pedophiles, and pedophilia? I am going to run with two scenarios. There are more, but I think two are sufficient to make my point about pedophiles.
Ready?
Scenario One
So, a male friend comes to you and tells you that they are a pedophile, that they have sexual attractions to children. To you, a pedophile is someone who molests children. You ask him who the victim was. He says there was no victim. You are baffled, because a pedophile is someone that molests children. The conversation ends, rather awkwardly.
The scene rubs you the wrong way, so you ask some people about it. They tell you the guy always seemed creepy, and so you call the police and tell the police what he told you. You know this guy is always hanging out with this one kid, and after calling the police, you ask this one kid if the guy has ever touched him in an odd way. The kid says yes, he has. So the police come, you tell them what the child said, and the police interview the child. The child repeats that the guy has touched him in an odd way.
So the police arrest the guy, and the guy takes a plea deal and spends ten years on probation for molesting a child. Only… he does not finish his probation. His probation gets violated because he cannot find a job, and decides to talk to children anyway. He becomes sexual with one of them, and gets caught for molesting a child.
Scenario Two
Very similar to the first scenario, a male friend tells you they have pedophilia, and they are a pedophile because they have pedophilia. You are shocked, and you want to know what pedophilia is, because it sort of sounded like he was emphasizing the fact that he had pedophilia.
So you pull out your phone, and you look up what pedophilia is, and you see on Wikipedia that it is:
A psychiatric disorder in which an adult or older adolescent experiences a primary or exclusive attraction to prepubescent children.
You go on to read that:
In popular usage, the word pedophilia is often applied to any sexual interest in children or the act of child sexual abuse. This use conflates the sexual attraction to prepubescent children with the act of child sexual abuse, and fails to distinguish between attraction to prepubescent and pubescent or post-pubescent minors. Researchers recommend that these imprecise uses be avoided because although people who commit child sexual abuse sometimes exhibit the disorder, child sexual abuse offenders are not pedophiles unless they have a primary or exclusive interest in prepubescent children, and the literature indicates the existence of pedophiles who do not molest children.
You sort through the academic gobbledegook and look up what sorts of sexual therapists there are in your area, and tell your friend… you are sorry he is facing that disorder, and you want to help however you can. You understand that a disorder is something that people do not choose and cannot help, and you want to be there for your buddy.
What Just Happened There?
What you just witnessed are two very different reactions to something that is really not very common: Someone telling you that they are a pedophile. Obviously in the first scenario, there is no attempt to verify what they are saying, there is just the assumption of what a pedophile is, and the inability of the pedophile in question to explain what they mean. Maybe they are a teenager, maybe they just do not have the words. But regardless, they now have to face stigma and hate for the rest of their life because an assumption was made, and it snowballed from there… and eventually a child was harmed.
That first scenario can play out any number of ways to come to that conclusion of a child being abused. Maybe instead of the police, the person tells someone who then blabs it to everyone they know, and then it goes on Facebook… and then his life is ruined because no one will hire him, no one will house him, and he eventually turns to children to cope with his stress. Regardless of how the pedophile goes from telling their secret to being under a tremendous amount of stress, that pressure needs an outlet, and there is the chance that the outlet becomes directed at children rather than themselves.
While many times this stress is indeed directed inwards (alcohol abuse, drug abuse, depression, anxiety, lack of friends… etc), it can sometimes be directed to others… and that becomes risky. It can be directed at children, or it could impact children by viewing images or videos where they are being sexually abused.
The second scenario… I fooled you. See, I set it up in a way that makes it seem like the friend did the right thing by looking up the term- which they did. However, they still found wrong information. While it is noted briefly in Wikipedia, pedophilia and pedophilic disorder are treated as two different things, and both are indeed separate from child sexual abuse.
Child sexual abuse is certainly an atrocity. But by knowing the difference between child sexual abuse, pedophilia, and pedophilic disorder, we can know how to react to each situation so that we can treat people in the best possible way. By knowing the essential information that can make all the difference in the world, we can ensure that we react properly to what we are being told… and correct others when they do not use the proper words to communicate what they mean.
But If Stress Can Be Directed Outwardly, Then…
Exactly: Not all child sexual abuse is perpetrated by pedophiles. It means that some people, who have never felt an attraction towards children in their life, can sexually abuse them. And this happens: In fact, it is more frequent than child sexual abuse that is perpetrated by pedophiles. One-third of sexual abuse is perpetrated by pedophiles, and two-thirds are perpetrated mainly by heterosexuals. So if we are to blindly judge sexual feelings as being a threat to children, then we must pin the blame firmly on heterosexuals, who make up two-thirds of abusers. See where blaming sexual abuse on sexual feelings leads? Nowhere in a hurry. So now what?
Child Sexual Abuse Is About Power, Control, And Self-Deception
Ifchild sexual abuse were about feeling pleasurably about being sexual with a child… we would expect rates of child sexual abuse to be much higher than they actually are. We know from researchers and therapists that the number of motivations and the full explanation for those motivations for child sexual abuse are vast enough to fill a fairly dense book. Even one of the best researchers in the field, Elizabeth Letourneau, was only able to narrow down the motivations for juveniles who sexually abuse children… into 19 basic items.
A list of 19 motivations is not simple to comprehend, and that is just the motivations for juvenile sexual abusers. Dr. David Finkelhor outlined a process by which someone breaks down the barriers to being sexual with a child into four basic steps, and his process is not simple either. Suffice it to say that grooming is just as much about breaking down the reluctance of the abuser as it is about the reluctance of the child.
The Best Way To Intervene
The best way to stop child sexual abuse, and intervene, is to act before the abuse happens. Some organizations advocate knowing the signs of grooming. Others focus on looking at the behavior of adults or older youth. Regardless, the focus needs to be on ensuring that those facing a significant amount of stress have the ability to handle it without taking it out on other people. We need to ensure that they have healthy self-care habits. This is true for people who react outwardly and those who react inwardly: If we can teach them how to manage the intense feelings that they are facing in a healthy way, then child sexual abuse and a variety of other ills can be reduced greatly.
Mental health is just as important as physical health.
Often, I get up in news discussions and say something to the effect of... "Most sex offenders do not reoffend, most sexual crimes are committed by first-time offenders, not registrants. Our money would be better spent on preventing these crimes before they can happen."
And someone says to me... "Right, that sounds great. But how do we do that?" So, I think it is high time to discuss some practical ways that people (yes, you) can prevent child sexual abuse, as well as systemic policies that can be put in place. In the midst of writing out the prevention section for the website, I think this deserves a blog post as well.
Remember That Symposium?
Remember that rather dry symposium I covered last month? Well, one of the presentations was by Jill Levenson, discussing among other things, the fact that most sex offenders have trauma in their backgrounds. So what, sex offenders had a rough childhood. Exactly. But here is the thing: If we know that most of them come from some sort of trauma in their childhood, we know early on who is at-risk to becoming a sex offender. If we can help take care of them and give them the message that they are loved, believed in, etc... then we can intervene before they hurt people. And it is not just sex offenders: Dr. Levenson's presentation had similar findings for crime in general, not just sex crime.
Interventions For At-Risk Youth
There does need to be formal interventions for children with traumatic childhoods, and without the label. Someone with a rough background does not need to hear that they are at-risk, I mean, really. But we do need programs to reach these children, and mentors as well. After-school programs, mentoring, and the YMCA have done a lot of good in these areas. Ministries aimed at youth have also done very well. So, there is a need for formal programs here.
But let me share a brief tale of when I was a camp counselor. My first week, I had a very diverse group of middle school kids, and one of the kids had me hearing things like "emotionally disturbed" and "anti-depression medication" and "lost his mom when he was eight." You get the idea, I am sure. Well, one day, some girls came up to me and told me that this kid was pushing them off the swing. So I go up to them all, and I tell them they need to get along or they will be in trouble. It was so effective that five minutes later, the camp director came up to me and told me that the kid would be sweeping the mess hall because he had kept doing it.
So, he and I are sitting there, waiting for the director to come and lecture him before he does his sweeping, and I ask if I could talk to him. He said no, he wanted to be left alone, so I respected that and kept silent. The director comes, and he sweeps, and we are walking back to all the other kids... and I asked him again if I could say something. I said to him, "I know you've had a rough life so far. I know you lost your mom, and I'm sorry about that. But please don't make the same mistake I did of taking it out on everyone else." I did not have any more problems with him the rest of camp.
This is just one story of many where I talked with youth going through a rough time. You do not need to be part of a program to make a difference. All you need to do is say a kind word, show that you care and understand, and tell them you believe in them. Kids need to hear that, even without trauma in their background.
Proper Sexual Education
One issue that needs resolving is that we teach children many, many things to help them succeed in the real world: Get a job, go to college, choose a career... but we do little to prepare children for sex and relationships. I was never taught consent growing up, the concept just was not taught. That is an issue, because children who are exploring with their sexuality can hurt younger children if they are missing the information they need to ensure they are safe and respecting others' boundaries.
We need comprehensive sexual education that goes beyond the physical and physical health aspects of sex: We need to teach consent, mental health, relationship health, respect, and everything in between. If we are going to prepare children for the real world, we must prepare them for how to handle sex and dating, and the potential legal consequences for not handling those areas well. We cannot just assume that they are moral enough to understand, because all the good intentions in the world can still cause harm without guidance.
Destigmatizing Mental Health
We need to talk about mental health and how we are feeling, and if we are parents, we need to demonstrate that to our children: Ask them how they are feeling, not just how they are doing. We need to talk about mental health, and we need to show children what self-care is. We need to stop stigmatizing mental health in our everyday speech: Calling something psychotic or retarded, referring to people as crazy, loony, or nutzoid... We need to stop using mental health as an excuse to bully people, and we need to stop pushing the issue under the rug or avoiding it altogether. For ideas in how you can start destigmatizing mental health in your sphere of influence, visit this website.
Using Proper Terminology
You had to know this was coming. Improper terminology can spread myths about sexual abuse that lead the public to erroneously believing that individuals or situations that pose zero risk to children... do pose a risk. Sometimes, we refer to child sexual abuse as "child sex offending" and those who perpetrate it as "sex offenders." I argue that both terms are incorrect: When someone has been caught, they are unlikely to commit a new sexual crime, particularly if a child is involved, so referring to it as an ongoing event (offending) is mistaken, as is referring to someone as being a constant perpetrator (offender), because those who perpetrate child sexual abuse are rarely adjudicated offenders: They are those with no criminal record, trusted in the community. We cannot define people by their behavior, attraction, mental illness, etc. It runs the high risk of putting our focus on the wrong population.
Referring to those who have abused as pedophiles is inaccurate, then, because you are using a label that refers to someone with a sexual attraction to children and implying that attraction is the cause for their abuse of a child. It minimizes child sexual abuse and pushes pedophiles further from help by conflating their attraction with acting on it, when the two are separate. Referring to child sexual abuse as pedophilia is even worse because it directly conflates feeling with action. Pedophilia needs to only be understood as a sexual attraction to children.
Defund The Sex Offender Punishment Scheme
As most who sexually abuse children are first-time offenders and sexual recidivism among sex offenders is extremely low, we need to stop spending so much money on policies that attempt to address an issue that does not exist. Instead, our efforts on sex offenders would be better spent on rehabilitating and furthering their reentry into the community: Extend help, not fear and suspicion. This would not only help curb what little sexual recidivism there is, but would curb the proportionately higher rate of general recidivism. Incarceration should be reserved for particularly heinous cases where there is no remorse and multiple prior sexual offenses: Incarcerate those who pose a risk to the public, and rehabilitate those who do not pose that risk.
In other words, no more registry. No more public notifications. No more hype and drama when sex offenders are released. Spend that money on research and prevention, not useless tactics that put children at increased risk.
In case you missed the other parts for this series, please see part one, two, three, or five.
As a refresher...
So, What Is This Symposium?
The Moore Center Symposium is a "meeting of the minds" on the prevention of child sexual abuse. It offers professionals (and advocates) an opportunity to learn more about the issue of child sexual abuse and how it can be prevented. The Moore Center for the Prevention of Child Sexual Abuse is a subset of Johns Hopkins' Bloomberg School of Public Health, which is a major educational institution in Maryland that is well-known for its work in the public health sector (as its name should indicate). The Moore Center is currently being directed by Dr. Elizabeth Letourneau, who used to be the president of The Association for the Treatment of Sexual Abusers (ATSA), and is a researcher that studies a myriad of topics within the realm of sexual abuse prevention. I am watching these admittedly dry and boring speeches to pull the essential parts out and communicate them to you. If you want to view them yourself, by all means, just be forewarned that they are dry and can be triggering.
Beginning Introductions
The symposium starts with an introduction by Johns Hopkins' President, Ronald Daniels, regarding some of the reasons for the symposium and the keynote speaker at the symposium, Patrick McCarthy, who is the president and CEO of the Annie E. Casey Foundation, an organization that focuses on improving the lives of children in a variety of ways. Other speakers at the symposium were Dr. Elizabeth Letourneau, Dr. Bruce Taylor (an expert in criminology), and Jill Levenson (expert in sociology and social work), followed by a showing of the film Untouchable, which I have talked about on this blog before. Following the film, there is a panel discussion about the film and closing remarks by Stephen and Julia Moore, the founding donors of the Moore Center.
Jill Levenson's Speech
Her speech focuses on early adverse childhood experiences and the causes of sexual offending. She starts with a handy little comic to illustrate the need to move beyond myth and current policy practices around prevention, and suggests that we need to start thinking about prevention differently.
She then gives a disclaimer that she does not want to minimize the pain done to sexual violence victims, but that it helps to have an understanding of how sexual violence happens and inform interventions. She states that there are no sides, there is no contest, and that sexual abuse victim organizations and advocates and sex abuse preventionists are not on opposing sides: Everyone is on the same team, trying to stop sexual violence. I would hope that advocates for the primary prevention of child sexual abuse, who have either been victimized by abuse, perpetrated abuse and lament it, or of any background really, are included in her team.
Public Health Model Of Primary Prevention
She starts by showing a graphic from the CDC about primary prevention where there are five areas that the CDC suggests to stop sexual violence: Promote social norms of protection, support victims/survivors, create protective environments, provide opportunities to empower and support women, and teach skills to prevent sexual violence.
She then asks what is missing from the model: Perpetrator prevention, or preventing someone from becoming a perpetrator. That is the focus of her speech. She then gives a handy demonstration of the public health model, which has three focuses: On primary prevention of universal precautions first, on secondary prevention of at-risk populations, and lastly on tertiary prevention of reacting when the problem presents itself.
Note: A handy way to think of this would be the flu: It is best to handwash and cover your mouth/nose (primary prevention - before the flu), and barring that, it is best to stay away from those that might be sick or getting flu shots to those who are vulnerable (secondary prevention - focusing on at-risk populations). The last thing you would want to do with the flu is just do nothing and wait for it to happen and then take steps (tertiary prevention).
She then points out that our resources and policies are currently aimed the polar opposite from what you would expect: Rather than focusing on primary, secondary, and tertiary prevention in that order, we "flip the pyramid" by focusing on tertiary prevention first, secondary second, and primary prevention last. In other words, we focus first on foster care, delinquency programs, incarceration, and sex offender registries/policies, we focus second on programs for at-risk youth and families, and improving parenting, and lastly we focus on primary prevention like changing cultural messages, reducing social problems, and reducing adverse childhood experiences (ACE's).
Overviewing The ACE Study
The Adverse Childhood Experiences study was a collaboration with the CDC and other researchers looking at family dysfunction and its causes. They originally were looking at obesity, and were noticing that many with issues with obesity had early harmful experiences in their childhood, so they did a study of over 17,000 participants to look at background challenges like abuse, family conflict, or neglect.
The survey looked at abuse, household challenges, and neglect: In abuse, they found that 21% experienced sexual abuse, 28% experienced physical abuse, and 11% experienced emotional abuse. In household challenges, they found that 13% dealt with violence towards their mother, 27% dealt with substance abuse, 19% had mental illness in the family, 23% dealt with a separation or divorce, and 5% had an incarcerated family member. In neglect, they found that 15% experienced emotional neglect and 10% experienced physical neglect.
They found that 36% of their sample had zero ACE's, 26% had one ACE, 16% had two ACE's, 9% had three ACE's, and 12% had at least four ACE's. Those numbers are about to be very important, but notice that in the original ACE study, they found that the higher number of participants had lower ACE scores, and that percentage drops as you increase the ACE score.
In other words, at least 64% of the population had some sort of adverse childhood experience of some kind. These experiences seemed to be correlated with social issues like a disordered social environment or caretakers who are not equipped to protect them from harm.
The ACE's that people experience as evidenced in the study are just a small representation of what people actually deal with in their life. She discusses the two kinds of ACE's that people can suffer: Disadvantaged communities (discrimination, poverty, bullying, crime, and violence) and unexpected events (accidents, injuries, illness, death of loved ones, a natural disaster).
She discusses the three different kinds of issues that are correlated with various mental health problems: Chronic events, multiple events, and cumulative events. She goes on to talk about the lasting effects that ACE's can have on people: Health issues (diabetes, obesity, depression, STD's, heart disease, cancer, stroke, COPD, broken bones), behaviors (smoking, alcoholism, drug use), and life potential (graduation, academic achievement, lost time from work). The ACE study found that the higher the ACE score, the more issues that come up.
Dr. Levenson's Study: Looking At ACE's and Sex Offenders
Dr. Levenson was interested in these effects, and what the backgrounds of sex offenders might look like with the ACE study in mind. So she and a few others did a study on that (Adverse Childhood Experiences in the Lives of Male Sex Offenders, Levenson, Willis, and Prescott, 2014). What they found was that sex offenders had a much higher number of ACE's in their background than general population males in every single category they studied.
When they broke down how many ACE's the male sex offenders reported, they found that 15.6% of sex offenders had zero ACE's, 13.7% had one ACE, 12.8% had two ACE's, and 12.3% had three ACES, which so far is in keeping with the original ACE study: Higher ACE scores are associated with lower percentages. However, instead of finding a lower percentage than 12.3% for sex offenders with an ACE score of 4+, they found a whopping 45.7% did... compared to 9% for general (non-sexual) offenders.
She looked in two other studies (Levenson and Socia, 2015, Levenson and Grady, 2016) studies at the correlations between ACE's and five areas: Criminal versatility (different types of arrests), persistence (quantity of arrests), sexual deviance, sexual violence, and substance abuse. She wanted to know which ACE's correlated with which of the five areas, finding that more sex crime arrests correlated with domestic violence, child sexual abuse, and emotional neglect, and that more general arrests were associated with substance abuse, unmarried parents, and an incarcerated family member.
She also overviews a study that featured in the OJJDP Journal of Juvenile Justice (The Prevalence of Adverse Childhood Experiences (ACE) in the Lives of Juvenile Offenders, Baglivio at al, 2014, p. 6-23) looking at the prevalence of ACE's in juvenile offenders. They surveyed over 64,329 juvenile offenders in Florida finding that the lower the ACE score, the fewer offenders (male or female) who reported having them, and the higher the score, the more offenders report them, maxing out at three ACE's for males and four ACE's for females, dropping back down. This finding was again consistent with the previous three studies overviewed.
She goes on to describe the results of a new, not-yet published study, looking at a variety of demographics: Original CDC ACE study sample (pink), adult sex offenders (gray), juvenile sex offenders (orange), and juvenile non-sex offenders (blue) and found a similar trend to the previous studies. As the results are not yet published, I drew a proportionate graph:
Sex Offenders Had It Rough. So What?
The point to all this is that both adult and juvenile sex offenders have some sort of childhood trauma, in many cases multiple traumas, that may serve as the backdrop for sexual offending. That being the case, how can we form interventions to help children with these traumas to prevent abuse, prevent maladaptive behavior, and also begs the question... what effect does this trauma have on children, and how to children react? She proposes three basic responses: Fight, flight, or freeze. When this happens, there are multiple internal reactions within the brain.
She says that these ACE's can change the architecture of the brain to create stress hormones, and they become conditioned psychologically, socially, and behaviorally to be ready for the next stressor or threat, and this limits the growth in essential processing skills areas. In other words, these events start a domino effect in the brain that, if not interfered with, can have lifelong consequences for those with ACE's in their background.
These can form beliefs and themes that are unhealthy and can lead to cognitive distortions, mental illness, and damaging patterns of thinking. Those beliefs and themes affect behavior through internal impacts that lead to impeded self-regulation and relational skills, two essential areas to developing appropriate behaviors that do not hurt others.
No Excuses, But Understanding For Interventions
She emphasizes that prior trauma is no excuse for sexually violent behavior, and that the presence of ACE's can help understand how sexually violent behavior develops and thus how we can intervene. She suggests that these effects on children and the child's brain can lead to using sexual assault to meeting emotional and social needs.
In other words, ACE's that are chronic and continuous can lead to factors like distorted boundaries, distorted skills, reenacting trauma on others, turn to children that are less threatening, getting needs met through violence and power, or taught to act in certain ways. Summarized more simply, "Kids growing up in chronically adverse conditions who then later in life sexual offend are somehow using sex and sexual assault as the vehicle to meet psychological, emotional, and social needs." The point, again, is to understand why this behavior happens. She proposes that children raised in chronically traumatic conditions (ACE's) evolve: Just as mankind evolved, children from traumatic vs. healthy environments develop maladaptive vs. healthy behaviors.
She acknowledges that we know that there are children who do not grow up to abuse others despite horrific trauma, but that we need to shift our paradigm in our communities in how we look at policies so that those with trauma in their backgrounds can get the help and interventions they need.
How Do We Treat Trauma, And How Must Policy Change?
In wrapping up her speech, she looks at the trauma-informed approach from SAMHSA: Realizing the prevalence and impact of trauma, recognizing the symptoms of trauma, responding by including knowledge around trauma into policy, procedure, and practice, and avoiding re-traumatization.
They discuss trauma-informed care and how to treat people in light of prior trauma as a way to solve a wide variety of problems besides just sexual violence. She also suggests a top-down, bottom-up approach by policymakers and other leaders. She talks about the need for role-models and supportive people who believe in those with trauma in their backgrounds, and how immensely helpful it is to have supports for those with ACE's and the earlier the better, but also for adults. Make sure that those with trauma have access to role models, mentoring, and are exposed to adults and peers who believe in them.
She suggests that people need to feel a certain accepted, valued, connected, and empowered, and without that, they resort to crime, gangs, teen pregnancy, and self-medication. In order to counter that, we must make opportunities for attachments, meaningful pursuits, self-efficacy, and self-sufficiency.
She reinforces that while not every abused child becomes an abuser, those with ACE's are more likely to grow up to abuse others.
She goes back to the prevention pyramid from the first few slides and flipping the pyramid to focus on primary prevention, the need to teach respect, consent, and issues in creating solid gender roles, as well as focusing on secondary prevention for at-risk populations of trauma-informed care in helping those with ACE's. She also touches on tertiary prevention, which should be the smallest area of focus: Think about treatment, support, and accountability so that they can successfully lead a law-abiding life and be responsible citizens.
In case you missed the other parts for this series, please see part one, three, four, or five.
As a refresher...
So, What Is This Symposium?
The Moore Center Symposium
is a "meeting of the minds" on the prevention of child sexual abuse. It
offers professionals (and advocates) an opportunity to learn more about
the issue of child sexual abuse and how it can be prevented. The Moore Center for the Prevention of Child Sexual Abuse
is a subset of Johns Hopkins' Bloomberg School of Public Health, which
is a major educational institution in Maryland that is well-known for
its work in the public health sector (as its name should indicate). The
Moore Center is currently being directed by Dr. Elizabeth Letourneau, who used to be the president of The Association for the Treatment of Sexual Abusers
(ATSA), and is a researcher that studies a myriad of topics within the
realm of sexual abuse prevention. I am watching these admittedly dry and
boring speeches to pull the essential parts out and communicate them to
you. If you want to view them yourself, by all means, just be
forewarned that they are dry and can be triggering.
Beginning Introductions
The symposium starts with an introduction by Johns Hopkins' President,
Ronald Daniels, regarding some of the reasons for the symposium and the
keynote speaker at the symposium, Patrick McCarthy, who is the president and CEO of the Annie E. Casey Foundation, an organization that focuses on improving the lives of children in a variety of ways. Other speakers at the symposium were Dr. Elizabeth Letourneau, Dr. Bruce Taylor (an expert in criminology), and Jill Levenson (expert in sociology and social work), followed by a showing of the film Untouchable, which I have talked about on this blog before. Following the film, there is a panel discussion about the film and closing remarks by Stephen and Julia Moore, the founding donors of the Moore Center.
Copyright note: The images of this post are copyrighted to Johns Hopkins University, which I have emailed approval for.
Elizabeth Letourneau's Speech
Dr. Letourneau's speech starts with acknowledgements and a brief discussion of prior symposiums. The topic of her speech, as with Patrick's, was to focus on policy's impact on prevention. Her speech focuses on juvenile sex offender registration and notification policies. She starts by looking at how someone would ordinarily solve a problem using a public health approach. First, you would do "surveillance" to determine what the problem is, then you would do "risk factor identification" to determine the cause of the problem, then "intervention evaluation" of what works to solve the problem, and finally, you would "implement" or take action to solve the problem. In that order, of course.
She points out that many issues have been resolved using this model, such as violence, environmental issues, infectious diseases, etc... yet child sexual abuse does not use this model. Instead, policy reactions to child sexual abuse are focused around the idea that abusers are sexually and morally deviant and at high risk to abuse the rest of their lives. She counters this notion with an incomplete list of causes for harmful sexual behavior in juveniles:
Traumatized children reacting to their own abuse
Persistently delinquent teenagers
Otherwise normal adolescents acting experimentally but irresponsibly
Generally aggressive and violent youth
Immature and impulsive youth
Adolescents engaging in normal but illegal consenting sex
Youth who take what they want because they are indifferent to others
Youth imitating what they see in the media
Youth misinterpreting what they thought was mutual interest
Youth ignorant of the legality of their actions or the possible ramifications
Youth imitating what is normal in their family background
Youth who get a thrill out of violating the rules
Socially isolated youth who use younger children as substitutes for peers
Seriously mentally ill youth
Youth responding to peer pressure
Youth preoccupied with sex
Youth using drugs or alcohol
Youth who get swept away by a moment of sexual pleasure
Youth with sexual deviance problems
She also points out that sexual crimes committed by juveniles have less duration and severity than adult offenses, and that juveniles are highly responsive to evidence-based treatment. She points out the findings of a study done in 2016 (Quantifying the Decline in Juvenile Sexual Recidivism Rates, Michael F Caldwell, full text available). That study looked at 106 studies and 11,000 cases and found that the general recidivism rate for juvenile sex offenders from 1980-1995 was 34.47% and the sexual recidivism rate for that period was 10.3%. Contrasted to the period of 2000-2010, which found a 30% general recidivism rate and a 2.75% sexual recidivism rate, Dr. Letourneau highlights that recidivism rates have declined, and that 97% of juvenile sex offenders will not reoffend with a new sexual offense.
She points out that sexual recidivism among juvenile abusers almost never happens once a child has been caught. She also cites a study she and her colleagues did sampling all of the juvenile offenders in Maryland, Oregon, and South Carolina who were in the legal system and they have the same findings as the above study: 3% reoffend sexually. She highlights this as a single example for the plethora of other studies with similar findings on the subject.
She discusses the restrictions placed on juveniles, such as residential treatment programs, sex offender registration, public notification, residence restrictions, employment restrictions, and education restrictions. She states that 38 states subject children adjudicated as minors to sex offender registration, and all minors adjudicated as adults. She gives the example from a juvenile offender featured in a New York Times article. That offender, named Johnnie, was caught at age 11 receiving oral sex from his younger sister. From there, the mother contacted the police, and Johnnie was arrested, charged, and convicted, then sent to a residential treatment program for a year and four months. Then, he was required to register as a sex offender in Delaware and put on their public list: His first suicide attempt was 2 weeks after being publicly listed (just shy of age 13, if you did the math).
They list some of the requirements of sex offender registration to illustrate what it is like:
Verify registry information in person at a state or local police station
On the offender's birthday, register every 90 days (tier three offenders), 3 months (tier two offenders), or 6 months (tier one offenders).
Register in each jurisdiction where someone resides or works.
May be handcuffed or put into a cell while waiting for processing
A sign may indicate that the offender is at the "Sex Offender Registration Desk"
Adult offenders and juvenile offenders may be registered in the same place (children in the same room as adult sex offenders)
Agents that process registration can be in any frame of mind: Angry, sad, happy, etc.
Provide 75 separate pieces of information, like SSN, internet identifiers, email address, vehicle registration/description, addresses for residence, work, or school.
Must report any change within 3 business days
Registration may be distributed online, or released to schools and other child-centered organizations, or law enforcement only, depending on risk level.
Note/Aside: Is this reminding anyone of Nazi, Germany? I never watched many Holocaust movies, and this seems eerily familiar...
She talks about this young man being just one example out of many hundreds, and references a Human Rights Watch report on the subject.
One Study On Juvenile Sex Offender Registration And Notification
Then she overviews a study that she did with the funding and collaboration of several other researchers and organizations, and begins discussing the recent follow-up study she did with the same collaborators to expand on it. The aims of their study were to examine the effects of registration and notification on six domains: Mental health, victimization, feeling of safety, feeling of social support, behavior, and association with peers. The demographics of the participants were discussed: Most were male, and the sample size was between 200 and 300 with an average age of 15.1 years old. Most were attending school, and most were heterosexual.
She discusses characteristics of the offenses, and compared those who were required to register with those who were not and did an analysis to control for any differences between the two groups. Registered offenders were more likely to be older, have a formal charge/adjudication, have a victim, and be caucasian.
The results of their analysis, without and with controlling for demographic differences found a variety of impacts on each of the six domains they were studying. They found that registered offenders were more likely to have mental health issues like suicide attempts/thoughts, depression, anxiety. They also found that registrants were more likely to have been victimized by someone sexually, were less likely to feel safe, and that non-registered offenders felt less social support than registered offenders.
Does Juvenile Sex Offender Registration Work?
She then asks the question, if even with all the collateral consequences of juvenile sex offender registration, does registration still work? Does registration make anyone safer? The research answers with a resounding no: There is no baby in the bathwater of juvenile sex offender registration, and every published study (yes, every one- if you want to challenge Dr. Letourneau's claim, by all means) has found no evidence of preventative or positive effects from juvenile sex offender registration. Many studies, by contrast, have found unintended and even harmful effects on juvenile offenders. She points out that registration has nothing to do with the causes of child sexual abuse and does not fit the realities of adolescence.
She talks about how rare it is in research to find such consistent findings across research literature on a particular policy. She agrees with the findings of Patrick McCarthy in his own mission, and states that juvenile registration is a failed policy that must end. She states three points to support this assertion: That few US policies have such wide research consensus regarding the effectiveness of a policy, that registration is like youth imprisonment where the message is that registered youth are dangerous, feared, and worthless with no real future, and that holding children accountable and providing them with evidence-based treatment can reduce the likelihood of future offending where sex offender registration cannot reduce that likelihood.
She then discusses some of the progress that is being made nationwide towards reforming juvenile sex offender registration: On a federal level, the Attorney General dropped juvenile notification requirements from federal policy and as of last year permits discretion in the registration of juvenile sex offenders; On a state level as of last year, Oregon and Delaware have replaced automatic juvenile registration with discretionary policies; The State Supreme Courts of Ohio and Pennsylvania have ruled against some components of juvenile sex offender registration.
She closes by stating that the time has come to abandon juvenile sex offender registration as a failed policy.
So, this past week, my news feed has been blowing up with big-sounding news out of Australia. The claim is that they are about to put a big dent in "child sex tourism", which is such a bad term to be using. Just call it child sexual abuse overseas or something, can we? I mean, you do not want to legitimize that sort of thing.
What Is The Issue?
Anyway, the news is that they are working on a bill to invalidate the passports of child sexual offenders. And that may seem like a good idea, right? I mean, clearly, if there are 20,000 people who are child sexual offenders in Australia, and 800 of them traveled abroad in the last year, it is an issue. You know, even if only half of those travel to SE Asia, and half of THOSE (by now we are talking 200 people, 1% of the total) failed to notify authorities per the requirement of their registration. So, clearly, focusing on maybe 1-2% of those affected is going to make a big impact on child sexual abuse in SE Asia. Something is not right there.
Several outlets have reported the news in a variety of ways:
Australia Is Walking Down The Path Of The United States: Tertiary Prevention
I have covered this time and time again: Policies aimed at sex offenders are only ever effective on recidivists, because these policies are what we call "tertiary prevention." They are a way to stop those who have already acted from acting again. This seems important, until you look at the data: Sex offender recidivism is extremely low, and most sexual crimes are committed by first-time offenders, not registrants.
In other words, primary prevention methods, or methods of intervening before a sexual crime takes place, are always going to be far more effective at stopping sexual crime, and tertiary prevention methods are always going to be the least effective way to stop sexual crime. Focusing on sex offenders, which works as a political maneuver but not much else, does not protect children.
Issues In Asia
One of the issues related to this is that child sexual abuse is a very serious problem in Asia, particularly the Southeast portion including Cambodia, India, and the Philippines. One of the problems is claimed to be that people are visiting these countries specifically to sexually abuse children, both boys and girls. While this is certainly an issue, and one that appears to be normal and accepted in these cultures (ie, it happens to everyone, not that people are okay with it), I very much doubt that this issue stems from travelling convicts with sex crimes on their record, because of the statistics I have seen. If that is not an issue in the United States (and the State Department has been on record saying that exact thing), then I doubt that other countries that are less wealthy than the United States have an issue either. Rather, the problem would be those who have no criminal record, some of whom are on business trips and dealing with job-related stress. It would be interesting to do a study on this issue, to see what kind of demographics are at play, but the proposal in Australia, similar to International Megan's Law in the United States, seems based more on politics than it is in actually keeping children safe.
Even The Jacob Wetterling Resource Center Says This
Remember Jacob? Maybe you did not grow up in Minnesota, but much of the sex offender policies we have started with three victims: Jacob Wetterling, Megan Kanka, and Adam Walsh. Jacob Wetterling's sexual assault, kidnapping, and murder (that last revelation came last year) sparked the activism of Patty Wetterling in creating a sex offender registry as an investigative tool for law enforcement. Her activism started the Jacob Wetterling Resource Center, which recently suggested we need to stop spending money on sex offenders and start spending it on prevention.
Pedophiles Are Not The Same As Child Sex Offenders Are Not The Same As Sexual Abusers
As always, the news media is butchering terminology around this issue. A pedophile is not someone who has hurt a child, they are someone with a sexual attraction to children. Most with that attraction never abuse, and most who abuse do not have that attraction. A child sex offender is someone who has been caught for a sexual offense with a child: Caught, not someone who has perpetrated it. For the purposes of the article from Australia, this is an accurate term.
However, when we refer to those that hurt children, it is highly inaccurate to call them child sex offenders because most are not adjudicated (seen in the criminal justice system). Most have never been caught, and most are known and trusted in the community and unlikely to ever be caught. Without using accurate terminology around this issue, we spread myths, like the idea that sex offenders just keep hurting children, or the idea that all pedophiles are a threat to children. Those myths fuel harmful policies that do not protect children, and cause all kinds of collateral damage.